Case: RCT on Tooth #19
45-year-old female with complex medical history (anemia, ulcerative colitis, PTSD, GAD, etc.).
CC: Pain of unclear etiology.
Dx: Symptomatic irreversible pulpitis and symptomatic apical periodontitis.
Tx: RCT after informed consent regarding possible crack.
Outcome: Pain relief following treatment.
Reflection
Challenging diagnosis with unclear etiology. Access was complicated by pulp stones, which were successfully removed. Patient has remained asymptomatic since treatment.




Case: RCT on Tooth #32
50-year-old female, Hyperlipidemia, Prediabetes, NKA.
Dx: Pulp necrosis and symptomatic apical periodontitis with PARL.
Tx: Non-surgical root canal therapy (RCT)
Reflection
Tooth #32 was retained due to its role as an abutment for the patient's RPD, making preservation critical. Access was complicated by mesial tilt and a metallic crown misaligned with the root axis. Treatment relieved the patient’s symptoms and maintained prosthetic function.



Case: RCT on Tooth #8
37-year-old female, healthy, no medications, no allergies.
Dx: Pulp necrosis and asymptomatic apical periodontitis with PARL
Tx: Non-surgical root canal therapy (RCT).
Reflection
Pulp stones were noted in #8 and neighboring teeth but did not complicate access. Minor sealer puff observed; given the biocompatibility of BC sealer, prognosis remains favorable. Awareness of sealer behavior is important for long-term outcomes.




Case: RCT on Tooth #13
39-year-old female, Anxiety, PTSD, NKDA.
CC: Gross cavity on tooth #13
Dx: Pulp necrosis and symptomatic apical periodontitis with PARL.
Tx: Non-surgical root canal therapy (RCT).


Reflection
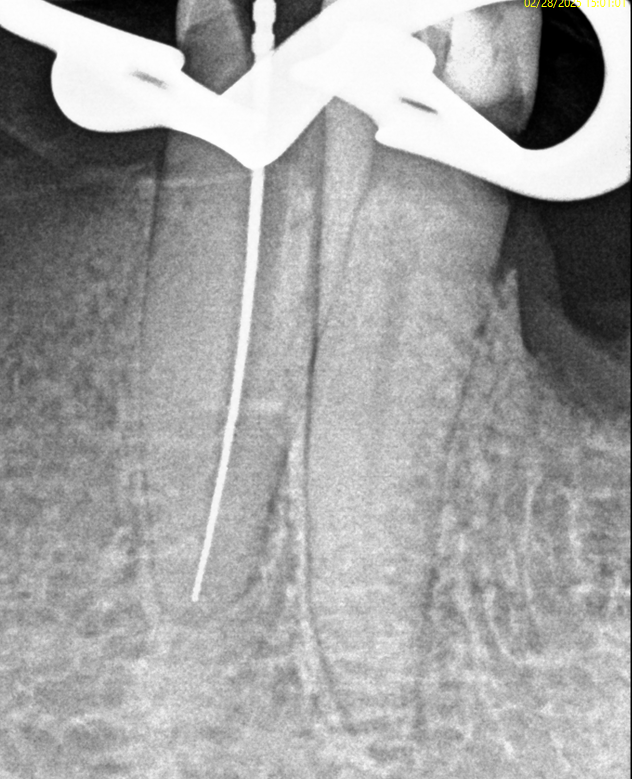
GP points were used to confirm the presence of a single canal. Apical root resorption complicated achieving an apical stop, leading to slight extrusion of gutta-percha. The patient was informed about the prognosis and the importance of follow-up monitoring.


Case: RCT on Tooth #6
58-year-old male, elevated LDL cholesterol, NKDA.
Dx: Pulp necrosis and chronic apical abscess.
Tx: Non-surgical root canal therapy (RCT).
Reflection
One of my earlier cases, this treatment reflects my growth in technique and clinical awareness. Access could have been more conservative, and a void is present in the obturation. Minor sealer extrusion was observed but is considered acceptable due to the biocompatibility of BC sealer.




Case: RCT on Tooth #6
54-year-old female, Anemia, Tinnitus, Sciatic nerve pain, Polyarticular arthritis, NKDA.
CC: Vague discomfort on upper right side, noted on biting.
Dx: Pulp necrosis and symptomatic apical periodontitis with PARL.
Tx: Non-surgical root canal therapy (RCT)
Reflection
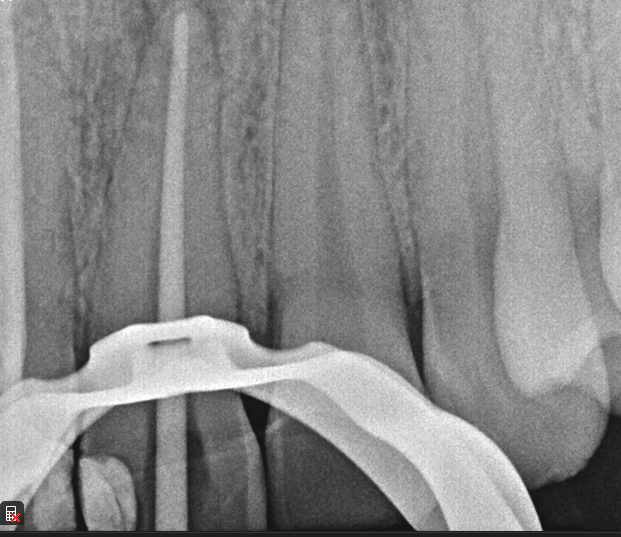
Long working length (29 mm) in a necrotic tooth required careful length control. Treatment was successful, and the patient remains asymptomatic.



Case: Regenerative Endodontic Procedure on Tooth #4
32-year-old female, pregnant, no medications, no allergies.
CC: "Hole in tooth."
Dx: Pulp necrosis and asymptomatic apical periodontitis with incomplete root development.
Tx: Regenerative endodontic procedure, patient elected regenerative approach over extraction.
Reflection
This case provided valuable experience in applying regenerative endodontic principles in practice. Although the patient's age presented a limitation based on current literature (preferably under 17), regenerative therapy was pursued to preserve the tooth. Challenges included achieving a semi-dry environment during the initial appointment and managing MTA placement at the second visit. The patient remains asymptomatic, and a 6-month follow-up is planned to monitor healing.






Case: RCT on Tooth #30
54-year-old female, osteoporosis (on oral bisphosphonate therapy), no known allergies.
Dx: Pulp necrosis and asymptomatic apical periodontitis.
Tx: Non-surgical root canal therapy (RCT).
Reflection
Given the patient's long-term bisphosphonate use (>5 years), root canal therapy was selected over extraction to minimize MRONJ risk, despite limited restorability. Treatment was complicated by a highly calcified and merging mesial root system. Patient remained asymptomatic and successfully proceeded with post and core buildup after two months.






Case: RCT on Tooth #21
49-year-old male, opioid dependence, chronic reflux esophagitis, NKDA.
CC: Pain
Dx: Likely symptomatic irreversible pulpitis; apical diagnosis presumed normal (pulp testing declined).
Tx: Root canal access; inflamed pulp observed.


reflection
This case highlighted the challenge of determining restorability in a structurally compromised tooth. Despite a guarded prognosis, the patient was insistent on saving it. Limited diagnostic testing also required reliance on symptoms and clinical findings, reinforcing the importance of flexibility and patient-centered care.

Case: RCT on Tooth #9
31-year-old male, healthy, no medications, no known allergies.
CC: Pain and swelling
Dx: Pulp necrosis and acute apical abscess (#9).
Extraoral: Upper lip fullness and tenderness.
Intraoral: Swelling and localized abscess.
Tx: Two-visit non-surgical root canal therapy with incision and drainage.


Reflection
This case involved managing both endodontic infection and acute swelling. The presence of facial swelling emphasized the urgency of drainage and systemic management. Coordinating I&D with RCT and pharmacologic support reinforced the value of staged treatment for optimal healing.

Case: RCT on Tooth #3
51-year-old male, healthy, no medications, no known allergies.
Dx: Previously initiated endodontic therapy and asymptomatic apical periodontitis #3.
Tx: Non-surgical root canal retreatment.


Reflection
This case emphasized the value of CBCT in confirming canal anatomy and avoiding unnecessary exploration. Completing treatment on an incompletely accessed tooth highlighted the importance of timely intervention to prevent chronic apical pathology.


Case: RCT on Tooth #8,9
49-year-old male, chronic abdominal pain, history of small bowel obstruction ×4, gastritis (treated), colitis, on famotidine. NKDA.
Dx: Symptomatic irreversible pulpitis (#8, #9); normal apical tissues.
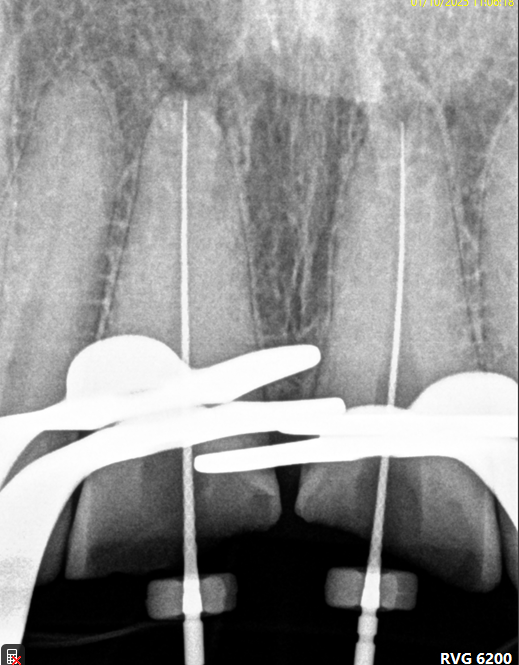
Tx: Root canal therapy due to pulpal exposure from severe occlusal wear.

Reflection
Restoring these teeth was questionable due to severe wear and limited vertical space. It was important to set expectations about the risk of not being able to place crowns afterward. The patient was still motivated to keep the teeth and chose RCT over extraction.


Case: RCT on Tooth #19
45-year-old male, schizophrenia, GERD, eczema, alcohol and methamphetamine abuse, antisocial personality disorder. Allergic to bananas and avocado. On ivermectin, furosemide, and omeprazole.
Dx: Pulp necrosis and symptomatic apical periodontitis without radiographic lesion.
Tx: Root canal therapy initiated.


Reflection
Managing this patient was tough. He was homeless, had psychiatric issues, and very low tolerance—he even walked out mid-treatment. But with patience and a flexible approach, we were able to complete the treatment. A good reminder that sometimes the biggest challenge isn’t the tooth, it’s the person in the chair.

Case: RCT on Tooth #9
13-year-old male, healthy, no medications, no known allergies.
Dx: Necrotic pulp and acute apical abscess (#9).
Tx: Root canal therapy initiated.


Reflection
This case involved a necrotic tooth with an open apex and blunderbuss canal. Achieving apical control was a challenge due to the lack of a natural stop. Apexification was considered, but we managed to adapt a large master cone (#60), trimming the tip to get a snug fit and achieve proper tug-back, allowing us to complete obturation successfully.


Case: RCT on Tooth #19
35-year-old female, Spanish-speaking, no past medical history.
Dx: Pulp necrosis and symptomatic apical periodontitis with PARL (#19).
Tx: Root canal therapy.


Reflection
The main challenge was the patient’s TMJ discomfort—she had trouble keeping her mouth open and needed multiple breaks. CBCT showed the mesial canals were converging apically, which helped guide shaping. Unfortunately, the distal canal appeared slightly overextended on the final image, reminding me of the importance of precise working length control, especially in cases with limited access.


Case: RCT on Tooth #9
67-year-old male, diabetes, no known drug allergies.
Dx: Pulp necrosis and chronic apical abscess.
Tx: Root canal therapy.


Reflection
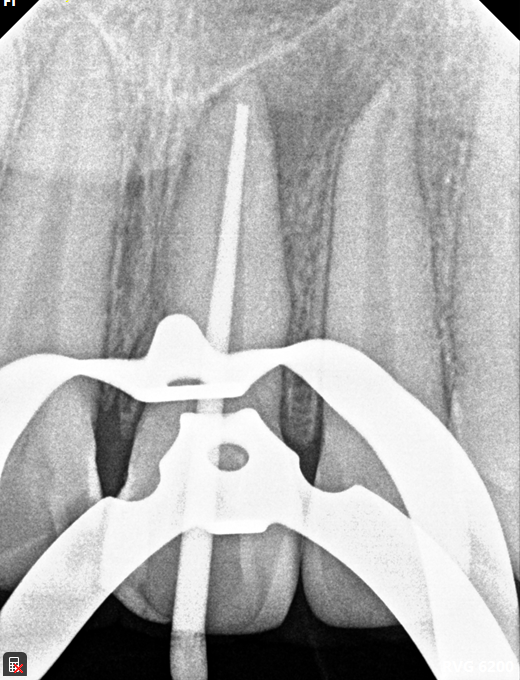
The main challenge in this case was negotiating calcified canals through an existing crown. Locating the orifice was difficult, but persistence paid off. The final X-ray showed a sealer puff from an accessory canal—right where the sinus tract had traced—suggesting thorough cleaning. With proper disinfection, we’re hopeful this will lead to healing of the fistula. The sealer puff is evident and, given its biocompatibility, not a major concern, though follow-up is essential.


Case: RCT on Tooth #8
33-year-old female, complex medical history including asthma, COPD, heart failure, fibromyalgia, anxiety, depression, ADHD, and chronic cough. NKDA.
Meds: Paroxetine, Sprintec, sumatriptan, albuterol
Dx: Previously initiated endodontic therapy and chronic apical abscess
History: Treatment was started in 2021 but not completed. The patient returned with pain following trauma (dog hit her face). Exam revealed a healed, non-traceable fistula on the attached gingiva
Tx: Root canal therapy.

Reflection
This patient has rampant caries and a high caries risk. She's on PreviDent and has received dietary counseling and intensive oral hygiene instruction. We had to pause the SMART caries management due to pain on #8. After managing the endodontic issue, a post space was prepared for future post, core, and crown. Temporary restorations were placed, and we’ll continue SMART therapy once she's more stable.

Case: RCT on Tooth #8
46-year-old male with a medical history significant for pituitary deficiency following brain surgery. NKDA.
Meds: Desmopressin, Levothyroxine, Prednisone, Somatropin, Testosterone
Dx: Asymptomatic irreversible pulpitis and asymptomatic apical periodontitis
Tx: Root canal therapy.


Case: RCT on Tooth #29
19-year-old male with no significant medical history. NKDA.
Meds: None
Dx: Necrotic pulp with chronic apical periodontitis (#29); external root resorption noted
Tx: Root canal therapy


Reflection
Tooth #21 also has had the cervical external root resorption. This case emphasized the importance of early detection in managing external root resorption. While #29 required RCT due to pulpal necrosis, #21 was identified early and successfully treated with a restoration, preserving vitality.

Case: RCT on Tooth #8
19-year-old with no significant medical history, NKDA, not taking any medications
Dx #13: Previously initiated endodontic therapy with symptomatic apical periodontitis
Tx: Non-surgical root canal therapy (nsRCT)


Reflection
Our approach is focused on understanding your needs and providing practical solutions. From personalized consultations to hands-on assistance.


Case: RCT on Tooth #19
14-year-old male
Medical History: No significant findings (no medications, no allergies)
CC: None reported; referred due to radiographic findings on tooth #19
Dx: Pulp necrosis, Chronic apical abscess
Tx: Non-surgical root canal therapy (RCT) completed on tooth #19

Reflection
Locating the mesio-buccal canal presented a challenge due to calcification, requiring careful exploration and magnification. Additionally, a large periapical lesion was noted on the radiograph. The extent of the lesion highlights the importance of long-term follow-up to monitor healing and confirm resolution.


Case: Root Canal Therapy on Tooth #3
Patient: 13-year-old female
Medical History: No significant findings (no medications, no allergies)
CC: Gross cavity on tooth #3
Diagnosis: Pulp necrosis with symptomatic apical periodontitis associated with a periapical radiolucency (PARL)
Treatment: Non-surgical root canal therapy (RCT) completed
Reflection
Access was smooth. CBCT and clinical exam confirmed absence of MB2, which was unexpected. Challenges included a young tooth with thin walls, lack of apical stop, and working length management in long and curved roots (palatal 24 mm, curved MB). Obturation could be improved. Additional challenge: patient was a pediatric case.




Case: Root Canal Therapy on Tooth #14
Patient: 19-year-old female
Medical History: Pregnant, no known drug allergies (NKDA)
CC: Pain #14
Diagnosis: Symptomatic irreversible pulpitis and symptomatic apical periodontitis without PARL
Treatment: Non-surgical root canal therapy (RCT)
Reflection
Access and treatment proceeded smoothly; absence of MB2 confirmed clinically and via CBCT. Septocaine was avoided due to pregnancy. Special attention was needed for patient positioning to ensure comfort and safety during treatment.




Create Your Own Website With Webador